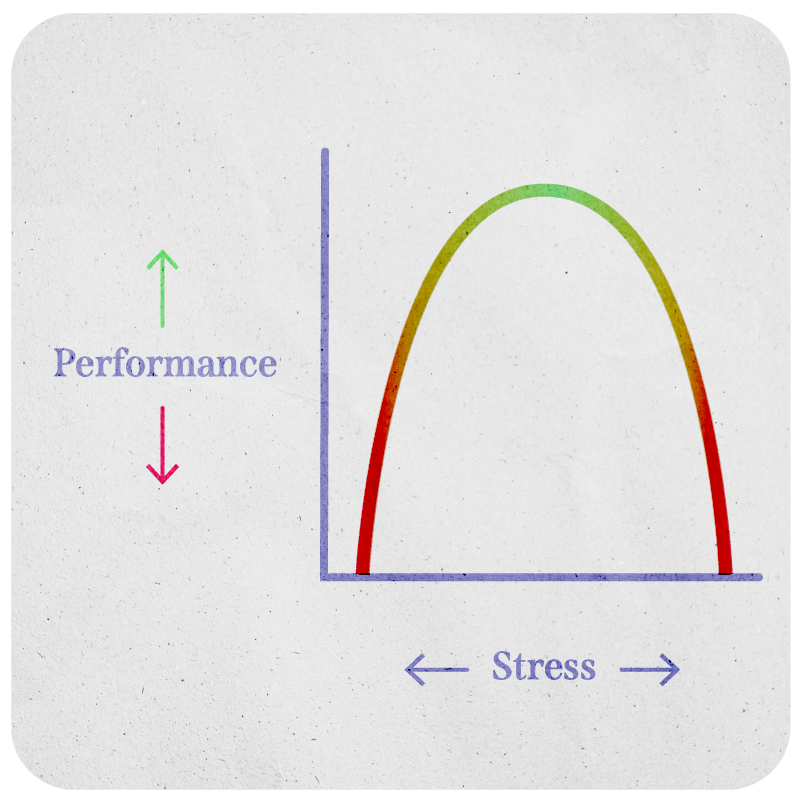
The association between the level of stress and mind-body performance is represented as an inverted U-shaped curve (Yerkes-Dodson law). Initially, the higher the stress, the better the performance, until stress passes the apex of peak performance, at which point more stress impairs performance.
The Yerkes-Dodson Law
The accumulation of trauma and other stressors across the lifespan is known as allostatic load.
If stress is too high for too long, it becomes ‘toxic.’ Neuroendocrine stress responses become over-sensitized, which leads to changes in the function of the brain and organ systems.
Each individual cue is linked to a particular square, which represents the initial response pattern. Through CCT, we’ll create new responses, new squares, over time. Every new square gets layered on top of the previous ones so that the initial trauma-response square becomes a three-dimensional cube, with multiple layers representing different reaction patterns and response options.
The CCT Square becomes the CCT CUbE over time
It is important to emphasize that in CCT, we are not trying to change the original square—the initial response pattern—but to add more squares on top of that over time. The rationale for this is that the responses in the original square were adaptive at one point in time, they were protective, and they may even prove effective in the future in the case of additional trauma exposure, despite being maladaptive in some current contexts. Thus, it may be counterproductive to eliminate strategies that children feel can keep them safe; they might fight us on it.
Instead, through the creation of new responses in CCT, we are empowering children to come to their own conclusion about which responses best work for them, and in what situation. In other words, children come to the realization that the new responses work better than the old ones without us having to jump to immediately “fix” the old response. The resultant CUbE provides more options for choosing adaptive responses over maladaptive ones. Rather than focusing on “right” versus “wrong” responses, CCT aims to promote flexibility and adaptability in responses, depending on the situation.
Psychoeducation is a crucial part of CCT intervention with a child. It occurs in Session 1, after the assessment is completed, and should be conducted with both the child and caregiver.
For younger children, an additional session may be needed to convey this information better.
Goals of Psychoeducation
Help the child and the caregiver understand: – What trauma is and how it develops – The normal stress response – Trauma symptoms – Development of cues through classical conditioning
Give the child hope for healing and recovery
Introduce CCT treatment: – Components – Format – Expectations
Dr. Kletter explaining the stress continuum to Tasha and her mother
Tasha and her mother enter the room but stay standing near the door. Tasha’s dark eyes dart here and there—her anxiety is palpable.
“Hi Tasha, how are you doing today?” you ask warmly.
“Okay,” she shrugs.
You smile and motion Tasha and her mother toward their seats. “How has everything been since the last time we spoke?”
“Just stressed,” she mumbles. “As usual.”
“Okay. Well, today we were going to take time to talk about stress—what it is and how it develops. What do you think?”
Tasha returns your gaze, but doesn’t respond.
“I’d like to start by asking if you can describe to me what you think stress is.”
Tasha fidgets in her seat and scrunches her forehead. “Stress is, like… when you’re very worried?”
“Mm-hmm, tell me more. Can you give me an example of a time when you felt stressed?”
“I don’t know, I feel weird like that all the time,” Tasha blurts. “Ugh which can make me think I’m going crazy.”
You remain still.
Tasha sighs. “It’s like a tension. I can’t breathe, and I feel shaky. I don’t know, it’s upsetting because I don’t have any control over it.”
She looks away and crosses her arms. “Those are very common signs of stress,” you explain, “not something crazy or ‘weird.’ People can have many different reactions to stress: thoughts, or a feeling, or a physical sensation, or even behavior.” Tasha’s gaze continues to trace the ceiling. “Has there ever been a time when you experienced stress, but it was helpful to you?”
Tasha looks at you. “Helpful? I don’t think so…”
“You know, a small amount of stress, believe it or not, can actually do some good,” you say with a bright smile. “It can motivate us. It can help us adapt.”
“Well,” Tasha uncrosses her arms. “I guess at school, when I have a test…I get stressed about it, so I study to try to get an A.”
“That’s a great example! What if we think about the other extreme? What if you were studying too much for the exam? Staying up all night, and skipping breakfast to study?” Tasha turns her face to you with curiosity. “How do you think you’d do on the day of the test?”
“I’d… probably be too tired.”
“That’s right, and your brain might be totally fried, wouldn’t it? Even if you know the information.”
Tasha nods emphatically.
“So too much stress can also be bad for us,” you continue, producing a pen and notepad to hold up in front of Tasha. “Imagine stress as occurring along a curve. On one side, there’s a positive stress response, the beneficial kind. But then, on the other side, there’s toxic or traumatic stress.”
Tasha focuses intently on the paper.
“All that stress we carry adds up, like a weight that we call ‘allostatic load.’ Sometimes the weight of the allostatic load over time can get to be too much—there’s a limit to how much stress we can handle.”
“Allostatic load.” Tasha repeats to herself. “Is that what happened to me? My ‘allostatic load’ is too much?”
“That’s correct,” you answer softly. “You explained that you’ve had a few major things that happened in your life, with your uncle and your cousins. Those weren’t normal day-to-day stressors. They were traumatic events. When those happen, they pile up and up until your mind and body tell you, ‘This is too much!’ So it makes total sense that this kind of compounding stress over time would eventually take a toll.”
“I don’t know,” Tasha mutters, “I wish I could be stronger.”
“Everyone’s limit is different. These things really depend on your biology and genetics, even past experiences. Some people are better at managing stress than others, sometimes because they’ve had more practice or help, other times because the people around them practice healthy coping. But none of this is to say that you’re doing a worse job than others.”
“I have a small assignment for you to do at home. Remember when we talked about cues?” you ask Tasha’s mom, as you pull out two sheets of paper. “I won’t see you again for a number of weeks—during that time I would like you to make a list of things you think might be cues for Tasha. Here are some examples.”
You hand her a sample list to look over. She skims it and hands it back. She asks, “So a cue could be something like how, every time we walk down the street where her uncle was killed, her heart starts to race?”
“That’s correct,” you nod in agreement. “The street is probably a cue. Be alert for things like that that Tasha seems to react to, or are connected with her feeling anxious or angry, that could be reminding her of her trauma. So anything like certain interactions, people, memories, or reminders.”
“Anything that I can think of?”
“That’s right. We want to write down as many potential cues as possible, and later we’ll review both your list and her list, so Tasha can pick a few to work on. By practicing those, she’ll learn to address other cues, as well.”
“Looks like I’ll be thinking about you even more than normal,” Tasha’s mother says to her daughter, with a wink and a nudge. Tasha smirks and looks away.
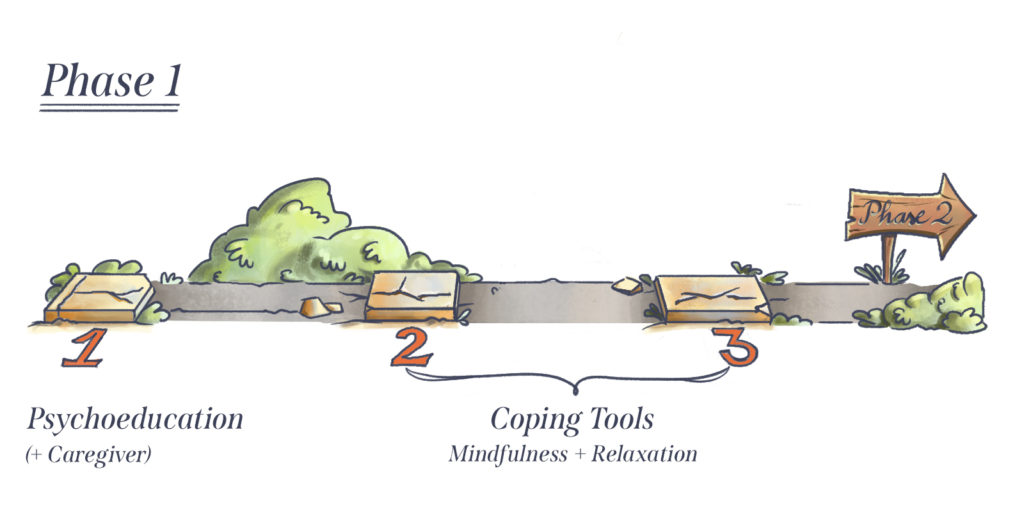
Cue-Centered Therapy consists of 15 sessions organized into four phases.
Describing this structure in Session 1 helps the child and caregiver know what to expect throughout the therapy.
Phase 1 provides the child and caregiver psychoeducation on stress, normal stress responses, PTSD, and cues. Coping tools are also introduced and practiced, in session and at home.
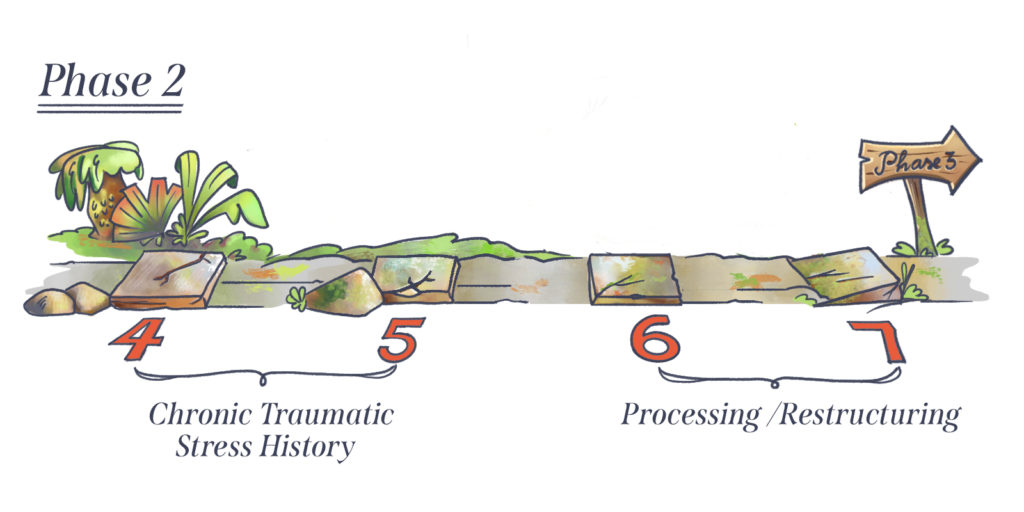
During Phase 2 (Sessions 4–7), the therapist helps the child build a life timeline to place traumatic events in the context of their entire life. The child also narrates their experiences of trauma. The therapist identifies emotions, cognitive distortions, cues, and memory gaps throughout the story. The therapist then helps the child process their experiences and restructure cognitive distortions identified in the story.
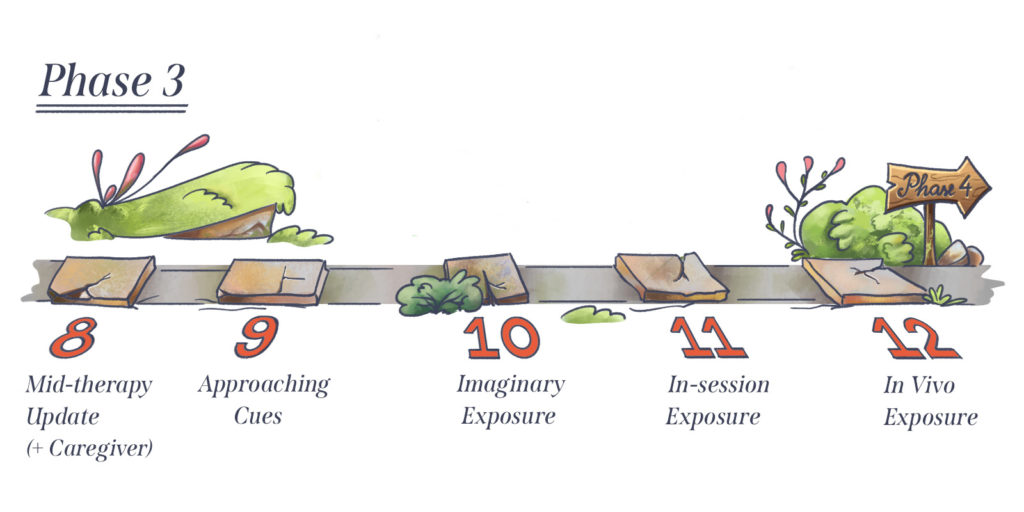
Phase 3 (Sessions 8–12) focuses on exposure to the identified cues using the coping tools that have been introduced in Phase 1. The exposure is practiced in gradual steps starting with preparation followed by imaginary, in-session, and in vivo exposures.
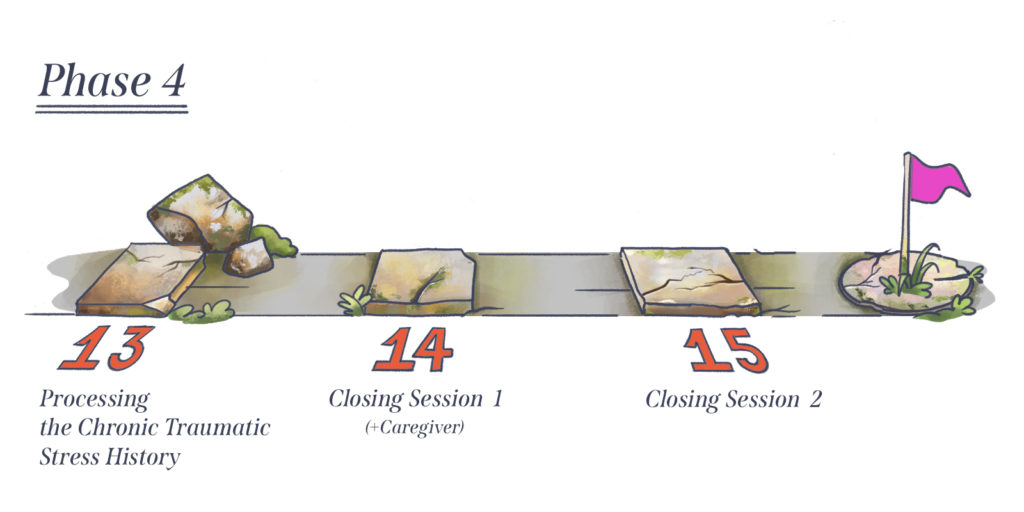
In Phase 4 (Sessions 13–15) the child integrates skills learned to revisit their trauma experiences. The therapist, child, and caregiver work together to ensure the sustainability of treatment benefits, and celebrate the therapeutic work.